
Should we really be vaccinating children against Covid?
Let’s have a look at some of the considerations
As we think about vaccinating children there are many considerations to take into account. The JCVI itself recommended against vaccines for the 12-15 age bracket considering that the risks outweighed the benefits. Now the US is pushing vaccines on children aged 5-11 and possibly even lower. As individuals consider the question of vaccinating their children, and as the UK might consider going down the same route, I thought it was important to bring together some research that sheds a different light on the matter.
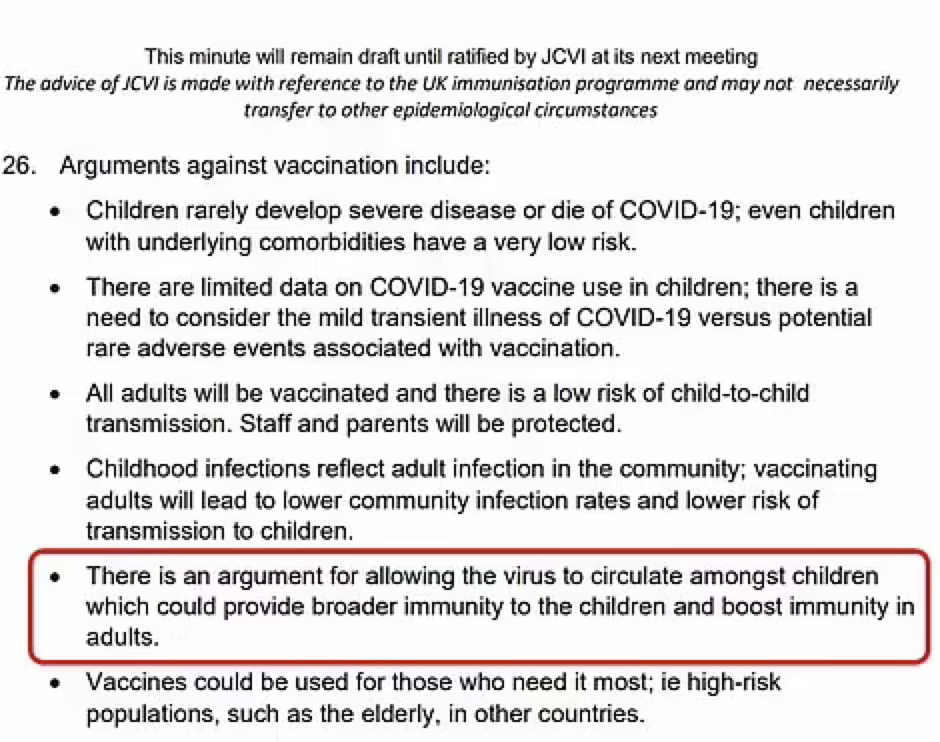
Below is an excerpt from the minutes of a JCVI meeting held on 13 May ’21
In this piece I will address a few questions pertaining to the risk of COVID for children: why their immune systems handle it so well, the risk/benefit of vaccines (using Pfizer vaccine as an example) and the case against vaccinating children from both the individual and public health perspective.
Risk of Covid in children
“Between March 2020 and Feb 2021, 3105 people under 18 died in England and Wales. Among those were 25 deaths from Covid. Half of those children had underlying complex conditions with high health-care needs, such as tube feeding or assistance with breathing.”
(https://www.nature.com/articles/d41586-021-02423-8)
There are 12 million children in England and Wales. Statistically this means that out of every 1 million children in England and Wales, 2 children died from Covid. Half of these will have complex healthcare needs and the other half likely have other co-morbidities such as obesity (Interestingly there has been a dramatic rise in childhood obesity during the various lockdowns. 1 in 7 children are now obese (https://www.dailymail.co.uk/news/article-10207641/Childhood-obesity-hits-record-high-Covid-NHS-data-shows.html).
So from a statistical perspective the risk of children dying of Covid is very low.
Why is the immune system of children so much more effective when it comes to COVID?
Several factors are likely contributing, including a stronger innate immune response (as opposed to the adaptive immune response that vaccines stimulate), less inflammation and fewer co-morbidities.
https://www.nature.com/articles/d41586-021-02423-8
The JCVI states that “children might be better off catching COVID at a young age, when they are at low risk, so that they are less vulnerable in adulthood, as is the case with chicken pox and other viral infections” (minutes from JCVI meeting on May 13th 2021).
It is important to keep sight of this wider perspective and not give in to a knee-jerk reaction to the situation that provides us with a single solution (vaccines) at the expense of all other considerations. Such a reaction may result in significant collateral damage in the form of short and long-term adverse reactions (which have not yet been studied), and failure to address underlying risk-factors which impact on our general health and longevity. There are also huge socio-economic costs associated with the vaccine program.
Most importantly, the vaccine-only route may also fail to help us achieve our goal of minimising the suffering caused by COVID. The JCVI wishes to avoid the trap of overmedication, which we have fallen into so disastrously with antibiotics. There is great risk in taking a singular perspective and not allowing for a fuller, multi-perspectival approach.
The JCVI contextualises COVID within our knowledge of other viruses such as chicken pox. Taking a wider view when looking at our current situation by looking through evolutionary, and ecological lens allows us to better understand the natural course of an encounter between a virus and a new host. We need to understand how the relationship between the host and the virus moves through time (evolutionary) and space (ecologically). How this relationship evolves over time is largely mediated by the mutations of the virus (how it adapts to us) and our natural immune response (how we adapt to the virus). This progression that has occurred innumerable times since mammals and viruses first met millions of years ago involves viruses adapting to us by becoming more transmissible and less symptomatic and human immune systems recognizing the virus more swiftly and dealing with it efficiently without over-reacting. This process is inevitable, and we could be actively facilitating it (by supporting immune function for example) while protecting high-risk individuals (with vaccines, drugs, vitamin D and by addressing risk factors). Instead we have lost sight of the natural course of events and are engaging still with a warfare mentality.
Vaccine safety in children
Now let’s have a look at the specifics of the safety and efficacy of the vaccine when it comes to children. In doing this I am referring to US data drawn from Pfizer trials. As there have been no UK clinical trials. For the moment I will bracket the issue of Pfizer’s integrity when conducting clinical trials, which is highly suspect: (https://www.bmj.com/content/375/bmj.n2635 This is not an isolated incident; Pfizer has a long history of unethical marketing and even an illegal clinical trial conducted in Nigeria which resulted in the death of 11 children and disability to dozens.)
Below is a link to the data report from the trial their vaccine trial:
https://www.ifm.org/news-insights/covid-19-vaccines-in-phase-3-trials/#table
Since the beginning of the pandemic there have been 94 deaths in the US among children aged 5-11 with COVID having been diagnosed (though this does not necessarily mean the primary cause – it can be very hard to sort this out). There are 24.9 million children age 6-12 in the US in 2021 (https://www.childstats.gov/AMERICASCHILDREN/tables/pop1.asp). We don’t have a perfect age overlap but that gives us a rough indication that we might be looking at around 3-4 deaths from COVID per million. It’s worth noting that the US probably has the highest rate of childhood obesity in the world.
There are numerous issues with the trial:
- Pfizer concluded that the trial was a big success. The vaccine is very effective at preventing infection and 100% effective at preventing death! But then so was the placebo: no children died with or without vaccines. Neither were any children hospitalized in either group. As we have already seen, mortality among children from Covid is exceedingly rare, and the very small sample size in this trial (1461 children in the vaccine group and 714 children in the control group) means that you cannot draw any valid statistical conclusions about effectiveness. Severe illness is unlikely to have shown up in such a small trial, vaccine or no vaccine.
- With regards to adverse reactions, the trial shows a high rate of “normal” vaccine side-effects (sore arm and so on) but is not big enough for myocarditis, pericarditis, anaphylactic shock, blood clots, or other severe reactions, including death to show up. Nor was the trial conducted over a long enough period for long-term effects to show up.The typical Pfizer vaccine side-effects for adults are below:
For adults: Anaphylaxis 11.1/millions.
Bell’s palsy .2/1000 (Which is less 4x less than from infection).
Acute Myocarditis: 1:3000 to 1:6000 Men 16-24.
It’s worth remembering that adverse reactions to drugs are heavily under-reported. I’ve seen estimates that 5-10% of adverse reactions are reported. If children responded the same as adults then we can see quite a high number of individual children will experience severe side-effects.
- Multiply the chances of severe adverse reactions by several times if the child has natural immunity. A study in the UK has found that individuals who previously had a Covid infection, ie with natural immunity, and are then vaccinated have a greatly increased risk of side-effects (for Pfizer specifically: 2-9x chance of side-effects and 56% increase in adverse reactions requiring hospitalisation). It’s important to remember that some side-effects may not show up for years or be contributors to more complex multi-factorial health problems.
Though myocarditis appears to resolve within a few months it’s important to note that there may be risk to other tissues in addition to inflammation of the heart and that the effects may not be immediately apparent. Newly published researched has shown that mRNA vaccines trigger elevation of inflammatory markers associated with an increased risk of ACS (Acute Coronary Sydrome). 5 Year risk of an ACS event (which includes hear-attacks) was raised from 11 to 25%. (https://www.ahajournals.org/doi/10.1161/circ.144.suppl_1.10712) We have no idea how long these markers, signs of inflammation, will remain elevated. Is this a risk we want to take with low-risk individuals, particularly our children?
Does it make sense to treat individuals for a health concern that is not problematic to them? The age group itself is negligibly impacted by COVID (first of all children tend to be barely symptomatic when they catch Covid, and secondly natural immunity provides much better protection against future variants of the virus). The vaccine is likely to cause a higher incidence of adverse reactions than Covid infection would, which counters the potential benefits of vaccination.
Should we really indiscriminately vaccinate a million children to protect 2-4 children? Does this make sense taking into account the unknown risks? What about protecting the vulnerable instead? I suggest this would provide great benefit at very low risk and cost.
The other argument made for vaccinating children is in regards to reducing transmission to potentially at-risk individuals. However, it is well established that vaccines don’t prevent infection or transmission. A study int he Lancet demonstrated that the transmission in a household was as likely from a vaccinated as from an unvaccinated individual. Wether vaccinated or unvaccinated, an infected child will potentially transmit within their household. (https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00648-4/fulltext)
In either case they are likely to be asymptomatic. A child (or adult) with natural immunity will be more likely to “break the chain” of transmission with no need to account for immunity waning within as little as 3 months of vaccination.
Addressing the risk factors:
How about addressing the risk factors? Can we be bothered? Neither the media, nor the government, nor even the scientific journals do justice to this strategy. A striking example is vitamin D3 deficiency. A recent meta-analysis shows that a mortality rate close to zero could theoretically be achieved with adequate vitamin D levels. Such an intervention would have minimal cost and nearly zero risk, along with multiple side benefits, as low vitamin D3 is implicated in many health conditions. (https://www.mdpi.com/2072-6643/13/10/3596).
I have already mentioned the pandemic of childhood obesity and diabetes. Both of these are risk factors not just for COVID but for many other causes of mortality including heart disease and cancer.
Treating obesity and diabetes would dramatically reduce morbidity and mortality over the course of the lifetime with the added benefit of protection from COVID.
Obesity related illness costs the NHS 6 billion pounds per year. The NHS have allocated a paltry £6 million to treat 1000 obese children per year with a comprehensive pilot program. On the other hand, the cost of vaccinating all 12 million kids? £264 million in cash to Pfizer (that would account for just a single dose). That figure does not include the financial and human costs of adverse reactions. Would the money not be better spent on treating the obesity pandemic?
Intervention in childhood, before the children have developed diabetes, cardiovascular disease, cancer and other diseases associated with disrupted metabolism, would greatly improve quality of life for each and every child! When discussing this with my eight year old son he pointed out that “they get bullied,” so emotional harm needs to be considered as a risk factor of obesity as well.. Treating children for obesity now would further provide some inoculation against future pandemics.
We would simultaneously be cultivating resilience against future infections and reducing the burden of chronic disease on our healthcare system.
What about natural immunity?
Vaccination effectiveness wanes after 6 months. This means that we would have to vaccinate 5-11 year olds twice a year at that huge cost, and with many potential risks. Natural immunity to viruses generally last a lifetime, and is more effective in protection against new variants. Survivors in of the 1918 Influenza had strong natural immunity 90 years later in a study conducted in 2008. (https://pubmed.ncbi.nlm.nih.gov/18716625/). Adding to the case for natural immunity a study in Qatar has shown that severity of re-infection is vastly reduced compared to primary infection. Natural immunity reduced the chance of re-infection by over 85% and there was not a single case of severe infection or death. (https://www.nejm.org/doi/full/10.1056/NEJMc2108120?query=TOC). Vaccinating individuals with previous infection provides negligible added protection while dramatically increasing the risk of side-effects. (https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full).
Healthy food and lifestyle choices too, last a lifetime and apart from preventing severe outcomes when infected with Covid, have many additional benefits for mental and physical health.
Additionally there are evolutionary mechanisms by which vaccines can drive the evolution of new variants – this is logical: if the spike protein is what the vaccinated immune system recognises then the virus will evolve variants with different configurations of its spike protein – natural selection in action.
However, natural immunity responds to dozens of different viral antigens, thereby conferring greater protection. A herd of children with natural immunity will be less likely to be an evolutionary testing ground for new variants attempting to “escape” the vaccine.
By not putting selective pressure on viruses to escape vaccine induced immunity, we will help maintain effectiveness of the vaccines in high risk individuals.
Lastly, since we know that the vaccines are effective at preventing hospitalisation and death amongst vulnerable adults (keeping in mind that 95% of those that die have co-morbidities and an average age of 83,) AND we have a variety of effective treatments (including new drugs, old drugs such as Invermectin, vitamin D, Zinc, etc.), do we really need to be vaccinating children? I suggest that the risks are not worth the purported benefits. Furthermore, the financial and human resources could be used much more effectively to support other strategies that would have a benefit for COVID (reduced hospitalization and mortality) while also addressing other causes of suffering and illness and generally resulting in a better quality of life.
















